
Attention deficit hyperactivity disorder facts for kids
Attention-deficit hyperactivity disorder (ADHD), sometimes called attention deficit disorder (ADD), is a common brain difference. It makes it harder for some people to focus, control their actions, and stay still.
People with ADHD can do everything others can. Their brains just work a bit differently, making it tough to stay focused. Thoughts might jump from one thing to another. They can be very active and find it hard to sit still. Sometimes, they might act or make choices without thinking them through first. This is called being impulsive.
More people are diagnosed with ADHD in some countries than others. For example, more people in North America are found to have ADHD than in Africa and the Middle East. In the United States, about 1 in 14 children (7%) has ADHD. This includes about 1 in 10 boys (10%) and 1 in 25 girls (4%). It's possible more boys have ADHD, or that fewer girls get tested for it.
For some people, ADHD symptoms become less noticeable as they grow up. Sometimes, the symptoms even go away completely when they become adults.
Contents
Signs and symptoms
Common signs of ADHD include trouble paying attention, being very active (or restless in adults), and acting without thinking. Kids with ADHD often have a hard time with schoolwork and making friends. It can be tricky to tell the difference between normal levels of being active or not paying attention, and when these signs are strong enough to be ADHD.
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), symptoms must last for six months or more. They also need to be much stronger than what is normal for someone the same age. For people under 17, at least six symptoms of not paying attention or being too active/impulsive are needed. For those 17 or older, at least five symptoms are needed. These symptoms must show up in at least two places, like at home, school, or with friends. They must also make it harder to do well in daily life. Also, some symptoms must have been present before age twelve.
Causes
ADHD happens because of differences in how the brain develops and works. It is linked to how some brain chemicals, like dopamine and norepinephrine, work.
Genes play a big part in ADHD. If someone in your family has ADHD, you are more likely to have it too. About 70-80% of ADHD cases are linked to genes. The rest can be due to new gene changes or things that happen in a person's life that affect brain development. Very rarely, ADHD can also be caused by problems with chromosomes.
Diagnosis
ADHD is diagnosed by looking at a person's behavior and how their mind develops. Doctors also check to make sure other things, like medicines or other health problems, are not causing the symptoms. Often, a diagnosis starts after a teacher notices concerns. Doctors also get information from parents and teachers. Many tools can help diagnose ADHD, but a proper diagnosis needs a doctor's confirmation. They also use special rating scales and information from different people in various settings.
Some common rating scales used to help diagnose ADHD include the Achenbach System of Empirically Based Assessment (ASEBA). These include the Child Behavior Checklist (CBCL) for parents to rate their child's behavior. There is also the Youth Self Report Form (YSR) for children to rate themselves, and the Teacher Report Form (TRF) for teachers to rate their students.
In North America and Australia, doctors use the DSM-5 guidelines for diagnosis. In European countries, they usually use the ICD-10. Not many studies have looked at diagnosing ADHD in children younger than 7 years old.
Management
Managing ADHD usually involves counseling or medicines, or sometimes both. There are different ways to help with ADHD symptoms. Medicines can greatly improve long-term results, but they also have some risks.
Behavioural therapies
There is good evidence that behavioral therapies help with ADHD. They are often the first choice for those with mild symptoms or for preschool-aged children. These therapies can include: learning about ADHD, behavior therapy, cognitive behavioral therapy (which helps change thinking patterns), family therapy, and school-based help. They also include social skills training, help with organization, and parent management training.
Medication
ADHD medicines seem to help by affecting certain areas and networks in the brain. They usually do this by increasing the amount of brain chemicals like norepinephrine and dopamine.
Exercise
Studies show that exercise does not reduce the main symptoms of ADHD. This conclusion comes from looking at many studies. Different types of exercise were studied, like martial arts, treadmill training, and aerobic exercise. The results were not consistent, so experts say there isn't enough strong evidence that exercise alone is an effective treatment for ADHD symptoms.
Diet
Experts like the American Academy of Pediatrics do not recommend changing diets to treat ADHD. This is because there isn't enough strong evidence that it works.
Some studies found that less than a third of children with ADHD might see some improvement if they take certain supplements or eat less artificial food coloring. These benefits might only apply to children who are sensitive to certain foods or who are also taking ADHD medicines. There is a small amount of evidence that low zinc levels might be linked to ADHD. However, taking zinc supplements is not recommended unless a person has a proven zinc deficiency, which is rare in many countries.
Interesting facts about ADHD
- Experts think that, throughout the world, about one in twenty children (5%) has ADHD.
- ADHD is most common in children: fewer adults have ADHD.
- The first clear description of ADHD is credited to George Still in 1902. He gave a series of talks about it in London.
- ADHD was officially known as attention deficit disorder (ADD) from 1980 to 1987. Before the 1980s, it was called hyperkinetic reaction of childhood.
- Even though people with ADHD might struggle with tasks that take a long time to finish, they can often do very well on tasks they find truly interesting or rewarding right away.
Images for kids
-
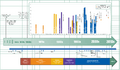
Timeline of ADHD diagnostic criteria, how common it is, and treatments.
-

The left prefrontal cortex, shown here in blue, is often affected in ADHD.
-

Percent of people 4–17 ever diagnosed in the US as of 2011



See also
 In Spanish: Trastorno por déficit de atención con hiperactividad para niños
In Spanish: Trastorno por déficit de atención con hiperactividad para niños
