
Ovarian cancer facts for kids
Quick facts for kids Ovarian cancer |
|
|---|---|
 |
|
| Micrograph of a mucinous ovarian carcinoma stained by H&E | |
| Symptoms | Early: vague Later: bloating, pelvic pain, constipation, abdominal swelling, loss of appetite |
| Usual onset | Usual age of diagnosis 63 years old |
| Risk factors | Never having children, hormone therapy after menopause, fertility medication, obesity, genetics |
| Diagnostic method | Tissue biopsy |
| Treatment | Surgery, radiation therapy, chemotherapy |
| Prognosis | Five-year survival rate c. 49% (US) |
| Frequency | 1.2 million (2015) |
| Deaths | 161,100 (2015) |
Ovarian cancer is a type of cancer that starts in the ovary. Ovaries are small organs in a female's body that produce eggs. This cancer can also start in nearby areas like the fallopian tubes or the inner lining of the abdomen.
Ovaries have different types of cells. When these cells become abnormal, they can grow out of control. They form lumps called tumors. These abnormal cells can also spread to other parts of the body.
At first, there might be no signs of ovarian cancer. Or the signs might be hard to notice. As the cancer grows, symptoms become clearer. These can include bloating, pain in the lower belly, and constipation. You might also notice your belly swelling or losing your appetite. Cancer can spread to the lining of the abdomen, lymph nodes, lungs, and liver.
Contents
Understanding Ovarian Cancer
What Causes Ovarian Cancer?
The chance of getting ovarian cancer goes up with age. Most cases happen after menopause, which is when a woman stops having periods. It is also more common in women who have ovulated more often. This includes those who have never had children. It also includes those who started ovulating younger or reached menopause older.
Other things that can increase risk include hormone therapy after menopause. Taking fertility medications and being overweight can also increase risk. Things that lower the risk are pregnancy and breast feeding. About 10% of cases are linked to genes passed down in families. For example, women with changes in the BRCA1 or BRCA2 genes have a higher chance.
How Doctors Find It
Doctors confirm ovarian cancer by taking a small piece of tissue. This is called a biopsy. The tissue is usually removed during surgery.
Treating Ovarian Cancer
If caught early, ovarian cancer can often be cured. Treatment usually involves a mix of surgery, radiation therapy, and chemotherapy. The outcome depends on how much the cancer has spread. It also depends on the type of cancer and other health conditions. In the United States, about 49% of women live for at least five years after diagnosis.
Ovarian Cancer Around the World


In 2020, about 313,000 women worldwide were diagnosed with ovarian cancer. In 2019, it caused 13,445 deaths in the United States. The number of deaths from ovarian cancer globally has increased since 1990.
Ovarian cancer is the second most common gynecologic cancer in the United States. It causes more deaths than any other cancer of the female reproductive system. Among all cancers in women, it is the fifth leading cause of death. The average age for diagnosis is 63. Deaths from ovarian cancer are more common in North America and Europe. They are less common in Africa and Asia.
Ovarian Cancer in the US


In 2022, about 19,880 new cases were found in the United States. Sadly, 12,810 women died from it. About 49.7% of women live for at least five years after diagnosis. Around 57% of cases have spread to other parts of the body when they are first found.
Ovarian cancer is the fifth most common cancer in women in the US. However, it is the fourth most common cause of cancer death.
Ovarian Cancer in the UK
In the UK, ovarian cancer is the 5th most common cancer in women. About 7,100 women were diagnosed in 2011. It is also the 5th most common cause of cancer death in women. About 4,300 women died from it in 2012.
Early signs are often mistaken for other common problems. These include bladder infections or irritable bowel syndrome. Many women in the UK wrongly think that cervical screening checks for ovarian cancer. This is not true.
Ovarian Cancer and Age
In the US, for women over 50, the rate is about 33 cases per 100,000. Ovarian cancer is most often found after menopause. This is usually between the ages of 60 and 64. Most cases (90%) happen in women over 45. About 80% happen in women over 50. Older women are more likely to have advanced cancer when diagnosed.
Ovarian Cancer During Pregnancy
Sometimes, ovarian tumors can happen during pregnancy. Doctors might find a lump during an exam or see a tumor on an ultrasound. These tumors are usually not cancerous. If they are cancerous, they often have not spread. Doctors can treat them with surgery. In some cases, chemotherapy might be needed.
What Scientists Are Researching
Scientists are always working to find better ways to detect and treat ovarian cancer.
Screening for Ovarian Cancer
Screening means testing people to find a disease early. For ovarian cancer, screening is not usually recommended for women with average risk. This is because current tests can often give false alarms. These false alarms can lead to unneeded surgeries.
However, scientists are trying to develop better screening methods. One idea is a test similar to the Pap smear used for cervical cancer. Another method combines blood tests with special ultrasounds. Researchers are also studying if screening helps women with gene changes like BRCA mutations.
New Treatments
Scientists are also looking into new ways to treat ovarian cancer. They are studying different types of medicines. Some medicines aim to stop the cancer from growing new blood vessels. Others are called PARP inhibitors. These show promise, especially for women with BRCA gene mutations.
Researchers are also studying hormone therapy and how to make treatments easier to handle. They want to help people deal with side effects like scar tissue from radiation. They also want to help with feelings like depression that can happen during treatment.
Clinical Trials
Clinical trials are studies where new treatments are tested. They help doctors find out if new treatments are safe and work well. These trials are important for finding better ways to fight ovarian cancer.
Images for kids
-

Age-standardized death from ovarian cancer per 100,000 inhabitants in 2004
-
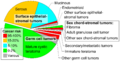
Ovarian tumors (including non-cancerous tumors) by incidence and risk of ovarian cancer.
-
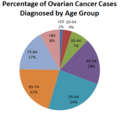
Ovarian cancer cases diagnosed by age group in the US
-
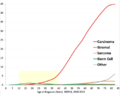
Ovarian cancer by age and type.
