
Pork tapeworm facts for kids
Quick facts for kids Pork tapeworm |
|
|---|---|
 |
|
| Scolex (head) of Taenia solium | |
| Scientific classification |
|
| Kingdom: | Animalia |
| Phylum: | Platyhelminthes |
| Class: | Cestoda |
| Order: | Cyclophyllidea |
| Family: | Taeniidae |
| Genus: | Taenia |
| Species: |
T. solium
|
| Binomial name | |
| Taenia solium Linnaeus, 1758
|
|
| Script error: The function "autoWithCaption" does not exist. | |
Script error: No such module "Check for conflicting parameters".
The Taenia solium, also known as the pork tapeworm, is a type of tapeworm. It belongs to a group of flatworms called cyclophyllid cestodes. You can find this tapeworm all over the world, especially in places where people eat pork.
Humans are the main hosts for this tapeworm. This means the adult worm lives inside humans. Often, pigs are the intermediate hosts. This means the young tapeworm stages live inside pigs.
Pigs can get the tapeworm eggs from human faeces (poop) that gets into their food. Humans can then get infected by eating pork that isn't cooked enough. This pork contains tiny tapeworm cysts. When pigs eat the eggs, they grow into larvae, then into oncospheres, and finally into these infective cysts. If a human eats a cyst, it grows into an adult worm in their small intestine.
There are two main ways humans can get infected. The first is by eating undercooked pork with cysts. This leads to adult worms in the intestines. Usually, people don't have any symptoms with this type of infection. It's also easy to treat with medicine.
The second way is by eating food or drinking water that has been contaminated with faeces from an infected person. This means you swallow the tapeworm eggs, not the cysts. These eggs develop into cysts mostly in the muscles. Most of the time, there are no symptoms. However, some people get serious symptoms, especially if the cysts form in the brain. This type of infection is harder to treat but still possible.
The adult tapeworm is flat and looks like a ribbon. It's white and can be 2 to 3 meters long, or even longer! Its tiny head, called a scolex, has suckers and a rostellum. These help it attach to the wall of the small intestine. The main body is made of many segments called proglottids. Each proglottid is like a small, self-contained unit that can reproduce. This is because tapeworms are hermaphrodites, meaning they have both male and female reproductive parts.
To find out if someone has the adult worm (primary infection), doctors often look for eggs in their faeces under a microscope. Sometimes, people notice shed segments of the worm. For the second type of infection (cysts in the body), doctors use imaging like CT scans or nuclear magnetic resonance (MRI). They can also test blood samples for antibodies using a special test called ELISA.
Taenia solium is a big problem in developing countries, especially in rural areas where pigs roam freely. How sick a person gets depends on how many parasites they have, their size, and where they are in the body. It also depends on how the person's body reacts to the parasite.
Contents
What is the Pork Tapeworm Like?
The adult T. solium is a three-layered worm with no body cavity. It's usually 2 to 3 meters long but can grow much bigger, sometimes over 8 meters! It's white and flat, like a ribbon.
The front end has a small, knob-like part called a scolex. This "head" is about 1 millimeter wide. The scolex has four suckers arranged in a circle around a part called the rostellum. These suckers help the worm stick to the host's intestinal wall. The rostellum also has two rows of spiny hooks made of protein. There are 22 to 32 hooks, some short (130 µm) and some long (180 µm).
After the short neck, comes the long body, called the strobila. The whole body is covered by a special skin called a tegument. This skin helps the worm absorb nutrients. It has tiny, finger-like parts called microvilli. The strobila is divided into 800 to 900 segments called proglottids. New segments grow from the neck area, so the oldest ones are at the very end.
There are three types of proglottids:
- Immature proglottids near the neck.
- Mature proglottids in the middle.
- Gravid proglottids at the end.
Since the tapeworm is a hermaphrodite, each mature proglottid has both male and female reproductive parts. The oldest gravid proglottids are full of fertilized eggs. Each egg is round and measures 35 to 42 µm across.
If fertilized eggs are released early in the human digestive system, they can develop into tiny larvae. These larvae then travel to form cysts (called cysticerci) in humans. There are three types of these cysts. The most common one is the "cellulose" cysticercus. It's a fluid-filled bladder about 0.5 to 1.5 cm long with a hidden scolex. Another type has a scolex, and the "racemose" type has no clear scolex but can be much larger. These can be 20 cm long and hold 60 ml of fluid. In some cases, people with brain cysts can have all three types.
-

Taenia solium adult
-

Taenia solium scolex (x400)
-

Egg of T. solium



What is the Life Cycle of the Pork Tapeworm?
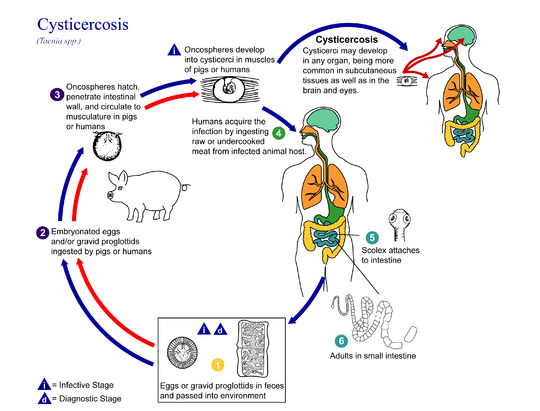
The life cycle of T. solium is a bit complex. It involves two hosts. The tapeworm passes from pigs (or other animals) as intermediate hosts to humans as definitive hosts. In humans, the infection can be short or last a long time, even for life if it reaches the brain. From humans, the eggs are released into the environment. There, they wait to be eaten by another host. In the intermediate host, the eggs develop into oncospheres. These bore through the gut wall and travel to other body parts, where they form cysts. These cysts can live for several years in the animal.
How Does it Live in Humans? (Definitive Host)
Humans get infected when they eat undercooked pork or other meat that contains the larval stage, called a cysticercus. Each tiny cysticercus is oval and contains a hidden scolex. Once inside the human small intestine, this scolex turns outwards. This process is helped by bile juice and digestive enzymes from the human body.
The T. solium then attaches to the upper intestine using its hooks and suckers. The suckers stick to the villi (tiny finger-like parts) in the intestine, and the hooks extend. The worm grows by taking nutrients from its surroundings. Its body gets longer as new proglottids form near the neck. In about 10–12 weeks, it becomes an adult worm. Adult worms can live for 2 to 5 years in humans.
Since it's a hermaphrodite, the tapeworm can reproduce by self-fertilisation (fertilizing itself). Or, if there are two worms, they can cross-fertilise by exchanging gametes between different proglottids. A full proglottid can hold over 50,000 fertilized eggs. These gravid proglottids often break open in the intestine, releasing the eggs in faeces. Whole proglottids can also be shed in groups. The eggs and detached proglottids spread through human defecation. These eggs can survive in the environment for up to two months.
How Does it Live in Pigs? (Intermediate Host)
Pigs are the most common intermediate hosts. They eat the eggs, usually from vegetation or water contaminated with human faeces. The eggs enter the pig's intestine and hatch into active oncospheres. The pig's digestive enzymes remove the outer layers of the egg.
Then, the oncospheres attach to the intestinal wall with their hooks. They use their own digestive enzymes to go through the intestinal mucosa and enter the blood and lymphatic vessels. They travel through the circulatory system to various organs. Many are filtered out by the liver. The ones that survive mostly go to muscles, but also to the brain, liver, and other tissues. There, they settle and form cysts called cysticerci. A single cysticercus is round, 1–2 cm wide, and contains a hidden scolex. The center is filled with fluid, like a bladder, so it's also called a bladder worm. Cysts usually form within 70 days and can keep growing for a year.
Humans can also accidentally become secondary hosts if they swallow eggs. This can happen if they get eggs from their own faeces (auto-colonisation) or eat contaminated food. Just like in pigs, the oncospheres hatch and enter the bloodstream. When they form cysts, it causes cysticercosis.
What Diseases Does the Pork Tapeworm Cause?
Signs and Symptoms
What are the Symptoms of Taeniasis?
Taeniasis is when the adult T. solium lives in the intestines. It usually causes mild or non-specific symptoms. These can include tummy pain, feeling sick, diarrhoea, and constipation. These symptoms appear about eight weeks after eating the infected meat, once the tapeworm has fully grown.
These symptoms can last until the tapeworm is treated and dies. If not treated, the infection can last for 2–3 years. Some infected people might not show any symptoms for years.
What are the Symptoms of Cysticercosis?
If you swallow T. solium eggs, or if egg-filled segments break open in your intestines, the larvae develop and travel into your body tissues. This causes cysticercosis. In pigs, it usually doesn't cause serious problems because they develop immunity. But in humans, infection with the eggs can cause serious health issues. This is because T. solium cysts often prefer to go to the brain.
If symptoms appear, they can include headaches, dizziness, and seizures. When the cysts infect the brain, it's called neurocysticercosis. This is a leading cause of seizures worldwide.
In more serious cases, people can develop dementia or high blood pressure. This happens if the cysts block the normal flow of cerebrospinal fluid in the brain. The severity of cysticercosis depends on where the cysts are, how big they are, and how many there are. It also depends on how the person's immune system reacts. Other symptoms can include problems with senses, uncontrolled movements, and brain problems. In children, eye cysts are more common than in other body parts.
Often, brain cysts can lead to epilepsy, seizures, damage in the brain, blindness, tumour-like growths, and low eosinophil levels. It can cause major brain problems like hydrocephalus (fluid buildup), paralysis, meningitis (brain swelling), convulsions, and even death.
How is it Diagnosed?
Stool tests are common. Doctors look at faeces samples under a microscope to find eggs. This is very accurate if the person doing it is trained, but it can miss infections if there aren't many eggs in the sample.
Stool tapeworm antigen detection: Using ELISA tests makes diagnosis more sensitive. However, these tests can be expensive and need special equipment and trained people. Some studies show these tests are very sensitive but only identify the general type of tapeworm, not always the exact species.
Stool PCR: This method can identify the exact species of tapeworm if material from a proglottid is taken from the stool. This method needs special labs, equipment, and trained staff. It hasn't been widely tested in real-world situations yet.
Serum antibody tests: These tests look for specific tapeworm antibodies in blood samples using methods like immunoblot and ELISA. These tests are usually very sensitive and specific. However, some studies show that commercial kits might not be as sensitive for certain types of brain cysts. The current best test for brain cysts is called LLGP-EITB.
It's hard for many developing countries to diagnose and treat this disease because they have limited resources. Many rely on clinical signs and imaging for diagnosis.
How Can We Prevent It?
The best way to avoid tapeworms is to not eat undercooked pork. Also, make sure vegetables aren't contaminated with faeces. Good hygiene and preventing faeces from getting into pig food are also very important.
You can prevent infection by:
- Properly getting rid of human faeces, especially near pigs.
- Cooking meat thoroughly.
- Freezing meat at -10 °C for 5 days.
For human cysticercosis, dirty hands are a main cause, especially among people who handle food.
How is it Treated?
Treating cysticercosis needs careful monitoring. This is because the dying worms can cause inflammation, especially if they are in the brain. Sometimes, doctors can remove the worms with surgery. In other cases, medicines like albendazole are given with steroids to reduce swelling.
For brain cysts, most patients who get medicine to kill the cysts see a big improvement in seizure control. Patients given both praziquantel and albendazole had better results in destroying the cysts. A study in 2014 showed that combining albendazole and praziquantel was more effective.
Scientists have also studied a vaccine to prevent cysticercosis in pigs. This could stop the parasite's life cycle in pigs, which would prevent humans from getting infected. However, using this vaccine on a large scale is still being considered.
Where is it Found? (Epidemiology)
T. solium is found all over the world. The two different forms of infection depend on whether people eat undercooked pork or swallow faeces-contaminated water or food. The full life cycle happens in places where humans live close to pigs and eat undercooked pork.
However, humans can also get the more harmful form (cysts in the body) by swallowing eggs. This happens in areas with poor hygiene, where faeces can contaminate food, soil, or water. High rates are reported in places with poor water hygiene and where pork is eaten, like Latin America, West Africa, Russia, India, and Southeast Asia. In Europe, it's more common in some Slavic countries and among travelers who aren't careful about eating pork.
The form where humans get cysts is common in areas where poor hygiene allows for slight faecal contamination of food, soil, or water. In the United States, immigrants from Mexico, Central and South America, and Southeast Asia have the most cases of cysticercosis. This is caused by eating tiny, tough tapeworm eggs. In West Africa, the rates of T. solium cysticercosis are not affected by religion.
For example, in 1990 and 1991, four people from an Orthodox Jewish community in New York City developed seizures and brain lesions. It was found to be caused by T. solium. All of them had housekeepers from Mexico, and some of these housekeepers were thought to be the source of the infections.
Neurocysticercosis causes about one-third of all epilepsy cases in many developing countries. Brain problems and deaths from this disease are still high in lower-income countries. They are also high in developed countries with many immigrants. We don't know the exact global numbers because screening tools, tests, and brain imaging are often not available in many affected areas.
Images for kids
-

Scolex (head) of Taenia solium
See also
 In Spanish: Lombriz solitaria para niños
In Spanish: Lombriz solitaria para niños
