
Wilms' tumor facts for kids
Quick facts for kids Wilms' tumor |
|
|---|---|
| Synonyms | Wilms' tumor Nephroblastoma |
 |
|
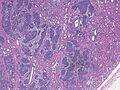
| High magnification micrograph showing the three elements of Wilms' tumor. H&E stain. | |
| Pronunciation | |
| Usual onset | 3–4 years old |
| Treatment | Nephrectomy Radiotherapy |
| Prognosis | ~90% of children are cured |
| Frequency | ~500 new diagnoses per year (United States) |
Wilms' tumor, also called nephroblastoma, is a type of cancer that grows in the kidneys. It mostly affects children, usually between the ages of 3 and 4. It is very rare for adults to get it. The tumor is named after Max Wilms, a German surgeon who first described it.
About 650 children in the United States are diagnosed with Wilms' tumor each year. Most of the time, it happens without any known genetic reasons. However, a small number of children with Wilms' tumor also have other health conditions they were born with. The good news is that Wilms' tumor responds very well to treatment. About 90 out of 100 children who get it are cured.
Contents
What Are the Signs of Wilms' Tumor?
It's important to know the signs of Wilms' tumor. If you notice any of these, it's a good idea to talk to a doctor:
- A lump in the belly that doesn't hurt.
- Not wanting to eat much.
- Tummy pain.
- Fever.
- Feeling sick to your stomach and throwing up.
- Blood in the pee (this happens in about 20% of cases).
- High blood pressure (sometimes).
How Does Wilms' Tumor Develop?
Wilms' tumor can happen for different reasons. Sometimes, it's linked to changes in a child's genes. Other times, it happens without any clear genetic cause.
Many cases of Wilms' tumor start from something called "nephrogenic rests." These are tiny bits of kidney tissue that didn't fully develop before a baby was born. After birth, these small pieces of tissue can sometimes turn into cancer.
Most Wilms' tumors are found in only one kidney. Less than 5% of the time, they are found in both kidneys. These tumors usually stay in one place and don't spread across the middle of the belly. If the cancer does spread, it often goes to the lungs. If a Wilms' tumor breaks open, it can cause bleeding and spread cancer cells. This is why doctors need to be very careful when removing it.
Under a microscope, a Wilms' tumor usually has three main parts:
- blastema (very early kidney cells)
- mesenchyme (supportive tissue)
- epithelium (lining tissue)
Sometimes, the tumor can also contain other tissues like muscle, cartilage, or even bone. The tumor causes problems by pressing on the healthy kidney tissue around it.
Doctors also look at how the cells in the tumor appear. This helps them predict how the tumor might behave:
- Favorable – The cells look more developed and organized.
- Anaplastic – The cells look poorly developed and disorganized. This type can be harder to treat.
Genes and Wilms' Tumor
Scientists have found that changes, or mutations, in certain genes can be linked to Wilms' tumor. One important gene is called WT1. It's found on chromosome 11. About 20% of Wilms' tumors have changes in this gene. Most of these changes are passed down from parents, but some happen after birth.
Another gene called CTNNB1 (which makes a protein called beta-catenin) can also have changes in Wilms' tumors. This gene is on chromosome 3.
However, most children with Wilms' tumor do not have changes in these specific genes.
How Do Doctors Find Wilms' Tumor?
Most children with Wilms' tumor are brought to the doctor because a family member or doctor notices a lump in their belly that doesn't hurt. Sometimes, doctors find these tumors during regular check-ups for children who have certain health conditions that make them more likely to get Wilms' tumor.
To find out if it's Wilms' tumor, doctors will:
- Ask about the child's health history.
- Do a physical exam.
- Order blood and urine tests.
- Use imaging tests like ultrasound, CT scans, or MRI scans.
An ultrasound is usually the first test to see if there's a mass in the kidney. A CT scan or MRI gives more detailed pictures.
To be absolutely sure it's Wilms' tumor, doctors need to look at a small piece of the tumor tissue. However, usually, they don't do a biopsy first because there's a small chance it could spread cancer cells. Instead, in North America, doctors often remove the entire kidney (a surgery called a nephrectomy) right away. In Europe, they might give chemotherapy first, then do the surgery. The final diagnosis is made by examining the removed kidney tissue.
Staging Wilms' Tumor
After the tumor is found, doctors "stage" it. Staging helps them understand how much the cancer has spread. This helps them decide on the best treatment and predict how well the child will do. Staging is based on where the tumor is located and what the cells look like under a microscope.
There are five stages for Wilms' tumor:
Stage I: Localized and Removed
In Stage I (about 43% of cases), the tumor is only in the kidney and has been completely removed by surgery.
- The outside of the kidney is smooth.
- The tumor did not break open or get biopsied before surgery.
- No cancer cells are found in the blood vessels or nearby tissues.
- No cancer cells are left behind after surgery.
- No spread to lymph nodes.
Stage II: Spreading but Removed
In Stage II (about 23% of cases), the tumor has spread a little bit beyond the kidney, but doctors were able to remove all of it during surgery.
- No cancer cells are left behind after surgery.
- Cancer cells might be found in the blood vessels near the kidney or in the soft tissue around the kidney.
Stage III: Not Fully Removed or Spread Locally
In Stage III (about 20% of cases), the tumor could not be fully removed during surgery, or it has spread to nearby areas.
- The main tumor cannot be operated on.
- Cancer has spread to nearby lymph nodes.
- Cancer cells are found at the edges of where the tumor was removed.
- Tumor cells spilled into the belly during or before surgery.
- The tumor was biopsied before surgery, or some tumor spilled during surgery in the side of the body.
Stage IV: Spreading Far Away
Stage IV (about 10% of cases) means the cancer has spread to other parts of the body far from the kidney. This could be to the lungs, liver, bones, or brain. It can also mean cancer has spread to lymph nodes outside the belly area.
Stage V: In Both Kidneys
About 5% of Wilms' tumor cases are found in both kidneys at the same time. This is called Stage V. Doctors try to stage each kidney separately based on how much cancer is in each one.
Treatment and Outlook
The good news is that about 90% of children with Wilms' tumor are cured. How well a child does depends a lot on the stage of their tumor and the treatment they receive. Finding and removing the tumor early usually leads to the best results.
Doctors can also look at specific changes in the tumor's chromosomes (like 1p and 16q). If these changes are present, it means there's a higher chance the cancer might come back. This helps doctors decide if a child needs more intense treatment.
Sometimes, statistics might look a bit confusing, showing similar or even better outcomes for more advanced stages. This can happen because doctors might use stronger treatments for those stages, or it could just be random chance in the studies.
| Stage | Histopathology | 4-Year Survival Rate | Treatment |
|---|---|---|---|
| I | Favorable cells (younger than 24 months or small tumor) | 98% | Surgery only (often part of a study) |
| Favorable cells (older than 24 months or larger tumor) | 98% | Surgery + chemotherapy | |
| Diffuse anaplastic cells | 80% | Surgery + chemotherapy + radiotherapy | |
| II | Favorable cells | 98% | Surgery + chemotherapy |
| Focal anaplastic cells | 80% | Surgery + chemotherapy + abdominal radiotherapy | |
| Diffuse anaplastic cells | 82% | Surgery + chemotherapy + abdominal radiotherapy | |
| III | Favorable cells | 94% | Surgery + chemotherapy + abdominal radiotherapy |
| Focal anaplastic cells | 100% | Surgery + chemotherapy + abdominal radiotherapy | |
| Focal anaplastic (pre-surgery treatment) | 71% | Chemotherapy first, then surgery + radiotherapy | |
| Diffuse anaplastic (pre-surgery treatment) | 53% | Chemotherapy first, then surgery + radiotherapy | |
| Diffuse anaplastic (immediate surgery) | 67% | Surgery + chemotherapy + abdominal radiotherapy | |
| IV | Favorable cells | 86% | Surgery + chemotherapy + abdominal and lung radiotherapy |
| Focal anaplastic cells | 72% | Surgery + chemotherapy + abdominal and lung radiotherapy | |
| Diffuse anaplastic (immediate surgery) | 33% | Surgery + chemotherapy + abdominal and whole-lung radiotherapy | |
| Diffuse anaplastic (pre-surgery treatment) | 44% | Chemotherapy first, then surgery + abdominal and whole-lung radiotherapy | |
| Bilateral (V) | Overall | 80% | |
| Favorable cells | 87% | Chemotherapy first, then surgery (saving kidney if possible), then more chemotherapy/radiotherapy | |
| Focal anaplastic cells | 88% | Chemotherapy first, then surgery (saving kidney if possible), then more chemotherapy/radiotherapy | |
| Diffuse anaplastic cells | 42% | Chemotherapy first, then surgery (saving kidney if possible), then more chemotherapy/radiotherapy |
If Wilms' tumor comes back after treatment, the chance of survival for children with a standard risk is about 80% after 4 years.
Who Gets Wilms' Tumor?
Wilms' tumor is the most common type of kidney cancer in children. It affects about 1 in every 10,000 children worldwide before they turn 15. Children of African descent might have slightly higher rates of Wilms' tumor. As mentioned, it's most common in children aged 3 to 4 years, and most cases happen before age 10.
Some rare genetic conditions can increase a child's risk of developing Wilms' tumor. For example, children born with a condition called aniridia (where part of the eye is missing) have a higher risk because of certain gene changes on chromosome 11. For children with these known risks, doctors often recommend regular ultrasound screenings to check for tumors early.
History of Wilms' Tumor Treatment
In the 1950s, a doctor named Sidney Farber and his team made a big breakthrough. They found that by using an antibiotic called actinomycin D along with surgery and radiation, they could greatly improve the cure rates for Wilms' tumor. Before this, about 40% of children were cured, but with the new treatment, it jumped to 89%!
In the early 1970s, an Italian doctor named Mario Costici realized that CT scans could be very helpful for diagnosing Wilms' tumor. This new imaging method made it easier to see the tumor and plan the best treatment.
See also
 In Spanish: Tumor de Wilms para niños
In Spanish: Tumor de Wilms para niños
- Hemihypertrophy
- National Wilms Tumor Study Group (NWTS)
- Perlman syndrome
- Virtual Karyotype for 1p and 16q LOH
Images for kids
-

Cut section showing two halves of a nephroblastoma specimen.
-
Low magnification micrograph of a Wilms' tumor infiltrating the renal parenchyma.


