
Vitamin D deficiency facts for kids
Quick facts for kids Vitamin D deficiency |
|
|---|---|
| Synonyms | Hypovitaminosis D |
 |
|
| The normal process of Vitamin D absorption | |
| Symptoms | Usually asymptomatic |
| Complications | Rickets, osteomalacia, other associated disorders |
| Causes | Lack of vitamin D, inadequate sunlight exposure |
| Risk factors | Age, people with dark skin, obesity, malabsorption, bariatric surgery, breastfed infants |
| Diagnostic method | Measuring the concentration of calcifediol in the blood |
| Prevention | Sufficient sunlight exposure, dietary intake |
| Treatment | Supplements |
| Medication | Cholecalciferol, ergocalciferol, calcifediol |
| Frequency | Severe deficiency (<30 nmol/L): Europe 13%, US 5.9%, Canada 7.4%. Deficiency (<50 nmol/L): Europe 40%, US 24%, Canada 37% |
Having Vitamin D deficiency means your body doesn't have enough vitamin D. This often happens when you don't get enough sunlight, especially sunlight with special UVB rays. Vitamin D is super important because it helps your body use calcium to build strong bones.
When you don't have enough vitamin D, your bones can become soft. This can lead to conditions like rickets in kids, which affects how bones grow. In adults, it can make bones weaker, increasing the risk of bone fractures. Vitamin D also helps your muscles work well.
You can get vitamin D from sunlight, as your skin makes it when exposed to UVB rays. Some foods like oily fish (salmon, herring) and mushrooms also have it. Many milks and other foods are also "fortified" with vitamin D, meaning it's added in. You can also find it in multivitamins.
| Top - 0-9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z |
What is Vitamin D and Why Do We Need It?
Vitamin D is a special nutrient that helps your body in many ways. Its main job is to help your body absorb calcium and phosphate. These are two minerals that are key for building and keeping your bones strong and healthy.
Without enough vitamin D, your bones can become weak and soft. This can cause problems like rickets in children. It can also make your muscles feel weak.
How Your Body Gets Vitamin D
Your skin can make vitamin D when it's exposed to UVB rays from the sun. This is why getting some sunlight is important.
You can also get vitamin D from certain foods. Good sources include:
- Oily fish like salmon, herring, and mackerel.
- Some types of mushrooms.
- Foods that have vitamin D added to them, like milk, some breads, and juices. This is called "fortified" food.
- Many multivitamins also contain vitamin D.
How Doctors Check Vitamin D Levels
Doctors usually check your vitamin D levels by doing a blood test. They look for a specific form of vitamin D called 25-hydroxyvitamin D. This gives them a good idea of how much vitamin D your body has stored.
Here's what different levels might mean:
- Severe deficiency: Less than 12 nanograms per milliliter (ng/mL).
- Deficiency: Less than 20 ng/mL.
- Insufficient: Between 20 and 29 ng/mL.
- Normal: Between 30 and 50 ng/mL.
Having normal vitamin D levels helps prevent bone problems and other issues.
Signs and Symptoms of Low Vitamin D
Often, people with low vitamin D don't feel any symptoms at all. It might only be found during a blood test. However, low vitamin D can cause or be linked to several health problems, especially with bones.
Bone and Muscle Problems
- Rickets: This is a childhood disease where bones don't harden properly. It can lead to bowed legs and other bone deformities. An early sign can be a soft skull.
- Osteomalacia: This is a bone-softening condition that affects adults. It can cause muscle weakness and fragile bones.
- Osteoporosis: This condition makes bones weak and brittle, increasing the risk of bone fractures.
- Increased risk of bone fractures: Weak bones break more easily.
- Muscle aches and weakness: Your muscles might feel sore or weak, and you might even have muscle twitches.
Other Health Links
- Periodontitis: This is a gum disease that can cause bone loss around your teeth, potentially leading to tooth loss.
- Respiratory infections: Some studies suggest that low vitamin D might increase the risk of getting severe breathing infections, including some types of COVID-19.
- Brain health: Low vitamin D levels have been linked to conditions like schizophrenia. Vitamin D is important for the normal development and function of your brain.
Who is at Risk for Low Vitamin D?
Some people are more likely to have low vitamin D levels.
Not Enough Sun Exposure
If you don't spend much time in the sun, or if you always cover up your skin, you might not make enough vitamin D.
- Sunscreen: While sunscreen is important for protecting your skin from sunburn, using a lot of it can reduce how much vitamin D your skin makes. However, in real life, most people don't apply enough sunscreen to completely block vitamin D production.
- Clothing: Wearing clothes that cover most of your skin can also limit how much sun your skin gets.
- Location: If you live far from the equator (like in the UK or Canada), the sun's rays are weaker in winter. This means your body makes less vitamin D during those months.
- Indoor lifestyle: Spending a lot of time indoors, whether for work or hobbies, means less sun exposure.
- Air pollution: In cities, air pollution can block UV light from reaching the ground.
Age
Older people are more likely to have low vitamin D. This is because their skin doesn't make vitamin D as easily from sunlight, and they might not get as much sun exposure.
Skin Color
People with darker skin have more melanin, which acts like a natural sunscreen. This means they need more sun exposure than people with lighter skin to make the same amount of vitamin D.
Body Fat
Vitamin D is stored in fat. People who are overweight or obese might have lower levels of vitamin D in their blood. This is because more vitamin D gets stored in their fat tissue instead of being available for the body to use.
Problems Absorbing Nutrients
Some health conditions can make it hard for your body to absorb nutrients from food, including vitamin D. These include conditions like celiac disease or inflammatory bowel disease. Surgeries that change how your intestines work, like some weight loss surgeries, can also affect vitamin D absorption.
Breastfeeding Infants
Babies who are only breastfed might need extra vitamin D. This is especially true if they have dark skin or don't get much sun. Doctors often recommend giving breastfed babies a daily vitamin D supplement.
How Vitamin D Works in Your Body
When your skin makes vitamin D from sunlight, or when you eat it, it's not immediately ready for use.
- First, your liver changes vitamin D into a form called 25-hydroxyvitamin D. This is the main form doctors measure in your blood.
- Then, your kidneys change 25-hydroxyvitamin D into the active form that your body uses. This active form helps your intestines absorb calcium from food.
If your liver or kidneys aren't working well, or if you have problems absorbing nutrients, it can affect how your body uses vitamin D. When your body doesn't get enough calcium because of low vitamin D, it might start taking calcium from your bones to keep blood calcium levels normal. Over time, this can make your bones weak.
Treating Low Vitamin D
The good news is that low vitamin D can usually be treated.
Getting More Sunlight
Spending some time in the sun can help your body make vitamin D naturally. Your skin knows when it has made enough, so you can't get too much vitamin D from sunlight.
Taking Supplements
Many people take vitamin D supplements, which are pills or drops that contain vitamin D.
- In the United States and Canada, recommended daily amounts are usually 400 IU for children, 600 IU for adults up to age 70, and 800 IU for people over 70.
- Babies who are only breastfed often need a daily supplement of 400 IU.
The amount of supplement you need depends on how low your vitamin D levels are. Your doctor will tell you the right dose. Sometimes, a higher dose is given at first to quickly raise levels, followed by a smaller daily dose to keep them up. Vitamin D supplements can be taken daily, weekly, or even monthly. It's often a good idea to take vitamin D supplements with a meal that contains some fat, as this can help your body absorb it better.
Vitamin K and Bone Health
Sometimes, vitamin D supplements are taken along with vitamin K supplements. This combination might help improve bone quality. Vitamin K can also help prevent calcium from building up in places it shouldn't, like in blood vessels.
History of Vitamin D Discovery
Scientists learned about vitamin D and its importance for bones a long time ago.
- Between 1918 and 1920, a scientist named Edward Mellanby found out that diet played a role in rickets.
- In 1921, Elmer McCollum discovered a substance in certain fats that could prevent rickets. Because it was the fourth vitamin found, it was named vitamin D.
- In the 1930s, milk in the United States started to be fortified with vitamin D. This helped greatly reduce the number of rickets cases.
Images for kids
-

Mapping of several bone diseases onto levels of vitamin D (calcidiol) in the blood
-
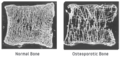
Normal bone vs. osteoporosis
-

Child with rickets



